CSF Otorrhea: Encephalocele and CSF Leaks
CSF leak of the temporal bone may occur spontaneously or result from trauma. Spontaneous leaks are rising in incidence, and are often associated with obesity, sleep apnea, and benign intracranial hypertension. The clinical presentation is often a unilateral clear effusion, and profuse otorrhea from a myringotomy tube. Occult leaks may present with meningitis. The diagnosis is established by sampling the middle ear fluid for beta-2-transferrin. Anatomic localization is obtained by CT scanning, which may demonstrate a bony defect in the tegmen or posterior fossa dural plate, and MRI, which may demonstrate an encephalocele. Temporal bone CSF leaks require surgical repair, and this may be performed through a transmastoid or transcranial approach. The latter is more reliable but has greater potential morbidity and longer hospital stay. Additional measures may be needed to reduce intracranial pressure.
- Recognize the clinical manifestations of cerebrospinal fluid (CSF) leak from the temporal bone.
- Summarize the medical conditions that contribute to spontaneous CSF otorrhea.
- Describe the radiologic methods of diagnosing and localizing CSF leaks.
- Review options for surgical management of temporal bone CSF leak and their risks and benefits.
Embryology
- Recognize the areas of potential congenital CSF fistulae in the temporal bone.
- Merchant SN, McKenna MJ. Neurotologic manifestations and treatment of multiple spontaneous tegmental defects. Am J Otol. 2000 Mar;21(2):234-9
- Wang B, Dai WJ, Cheng XT, Liuyang WY, Yuan YS, Dai CF, Shu YL, Chen B. Cerebrospinal fluid otorrhea secondary to congenital inner ear dysplasia: diagnosis and management of 18 cases. J Zhejiang Univ Sci B. 2019.;20:156-163
Anatomy
- Review the anatomy of the temporal bone and posterior and middle cranial fossae.
- Sen C, Chen CS, Post KD. Chapter 5, The petrous temporal bone. In: Microsurgical anatomy of the skull base. New York, Thieme, 1997. p. 83-101
Pathogenesis
- Summarize the risk factors for CSF leak.
- Explain the formation and drainage of CSF and the causes of intracranial hypertension.
- LeVay AJ, Kveton JF. Relationship between obesity, obstructive sleep apnea, and spontaneous cerebrospinal fluid otorrhea. Laryngoscope 2008;118:275–278
Incidence
- Cite the incidence of CSF otorhinorrhea in the general population.
- Identify the risk factors for CSF leak.
- Stucken EZ, Selesnick SH, Brown KD. The role of obesity in spontaneous temporal bone encephaloceles and CSF leak. Otol Neurotol. 2012;33(8):1412-7
- Kutz JW Jr., Husain IA, Isaacson B, Roland PS. Management of spontaneous cerebrospinal fluid otorrhea. Laryngoscope 2008;118:2195-2199
- Scurry WC Jr, Ort SA, Peterson WM, Sheehan JM, Isaacson JE. Idiopathic temporal bone encephaloceles in the obese patient. Otolaryngol Head Neck Surg 2007;136:961–965
- LeVay AJ, Kveton JF. Relationship between obesity, obstructive sleep apnea, and spontaneous cerebrospinal fluid otorrhea. Laryngoscope 2008;118:275–278
Patient Evaluation
- Describe the mechanisms of presentation of temporal bone CSF leaks.
- Explain laboratory methods of detecting and testing fluid for CSF.
- Gacek RR, Gacek MR, Tart R. Adult spontaneous cerebrospinal fluid otorrhea: diagnosis and management. Am J Otol 1999;20:770–776
- Nahas Z, Tatlipinar A, Limb CJ, Francis HW. Spontaneous meningoencephalocele of the temporal bone: clinical spectrum and presentation. Arch Otolaryngol Head Neck Surg. 2008;134(5):509-18
Measurement of Functional Status
- Recognize the relationship of intracranial hypertension and spontaneous CSF otorrhea.
- Schlosser RJ, Woodworth BA, Wilensky EM, Grady MS, Bolger WE. Spontaneous cerebrospinal fluid leaks: a variant of benign intracranial hypertension. Ann Otol Rhinol Laryngol 2006;115(7):495-500
- Brainard L, Chen DA, Aziz KM, Hillman TA. Association of benign intracranial hypertension and spontaneous encephalocele with cerebrospinal fluid leak. Otol Neurotol. 2012;33:1621-1624
Imaging
- Be familiar with the role and limitations of various imaging modalities for the diagnosis and anatomic localization of CSF leaks.
- Summarize the capabilities and pitfalls of different imaging techniques in surgical planning of CSF leak repair.
- Nelson RF, Hansen KR, Gantz BJ, Hansen MR. Calvarium thinning in patients with spontaneous cerebrospinal fluid leak. Otol Neurotol. 2015;36:481-5
- Reddy M, Baugnon K. Imaging of Cerebrospinal Fluid Rhinorrhea and Otorrhea. Radiol Clin North Am. 201;55:167-187
- Eljazzar R, Loewenstern J, Dai JB, Shrivastava RK, Iloreta AM Jr. Detection of CSF Leaks: Is There a Radiologic Standard of Care? A Systematic Review Detection of CSF Leaks: A Systematic Review. World Neurosurg. 2019 Feb 21. pii: S1878-8750(19)30434-6
Pathology
- Recognize the anatomic, radiologic, and pathological appearance of arachnoid granulations and arachnoid cysts.
- Recognize additional signs of intracranial hypertension.
- Gacek R. Arachnoid granulation cerebrospinal fluid otorrhea. Ann Otol Rhinol Laryngol 1990;99(11):854-62
- Remenschneider AK, Kozin ED, Curtin H, Santos F. Histopathology of Lateral Skull Base Defects. Laryngoscope 2015:125:1798-1806
Medical Therapies
- Identify the role of hyperventilation, medications, and other conservative measures in the treatment of CSF leak.
- Wang EW, Vandergrift WA 3rd, Schlosser RJ. Spontaneous CSF Leaks. Otolaryngol Clin North Am. 2011 Aug;44(4):845-56, vii
- Schlosser R.J., Wilensky E.M., Grady M.S., et al: Cerebrospinal fluid pressure monitoring after repair of cerebrospinal fluid leaks. Otolaryngol Head Neck Surg 2004; 130: 443-448
Pharmacology
- Describe the mechanism of action and expected response to diuretics, carbonic anhydrase inhibitors, and osmotic agents on intracranial pressure.
- Lueck C.J., and McIlwaine G.G.: Interventions for idiopathic intracranial hypertension. Cochrane Database Syst Rev 2009; 4: pp. 1-12
Surgical Therapies
- Explain the various transcranial, transtemporal, and combined approaches to CSF leak repair in the temporal bone, and their relative advantages and limitations.
- Describe the role of CSF shunting in the management of CSF leaks.
- Pelosi S, Bederson JB, Smouha E. Cerebrospinal fluid leaks of temporal bone origin: selection of surgical approach. Skull Base. 2010 Jul;20(4):253-9
- Oliaei S, Mahboubi H, Djalilian HR. Transmastoid approach to temporal bone cerebrospinal fluid leaks. Am J Otolaryngol. 2012 Sep-Oct;33(5):556-61
- Semaan MT, Gilpin DA, Hsu DP, Wasman JK, Megerian CA. Transmastoid extradural-intracranial approach for repair of transtemporal meningoencephalocele: a review of 31 consecutive cases. Laryngoscope 2011;121:1765-1772
- Carlson ML, Copeland WR, Driscoll CL, Link MJ, Haynes DS, Thompson RC, Weaver KD, Wanna GB. Temporal bone encephalocele and cerebrospinal fluid fistula repair utilizing the middle cranial fossa or combined mastoid-middle cranial fossa approach. J Neurosurg 2013;119:1314-1322
- Stevens SM, Rizk HG, McIlwain WR, Lambert PR, Meyer TA. Association between lateral skull base thickness and surgical outcomes in spontaneous CSF otorrhea. Otolaryngol Head Neck Surg. 2016:154:707-14
- Sanna M, Fois P, Paolo F, Russo A, Falcioni M. Management of meningoencephalic herniation of the temporal bone: personal experience and literature review. Laryngoscope 2009;119:1579–1585
Case Studies
Case 1. An 81-year-old gentleman complained of intermittent ear drainage from the left ear for about 25 years. He has had myringotomy tubes for most of that time, reinserted periodically. Without the tube, he had ear pressure and hearing loss. With the tube, he had drainage that was occasionally purulent. Cultures showed E.coli, Klebsiella, and corynebacteria. Various courses of oral and topical antibiotics did not relieve the drainage. On physical exam, the left eardrum was dull, and there was a patent myringotomy tube with scanty purulent drainage. CT scan showed fluid in the mastoid cells and soft tissue in the attic without scutal erosion (Figure 1).

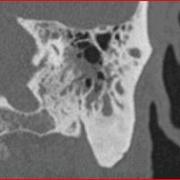
Figure 1
A mastoidectomy was recommended. At surgery, there was a small encephalocele protruding through a 4 mm tegmen defect (arrow, Fig. 2), with intermittent CSF leakage. The encephalocele stalk was fulgurated and the dura repaired with perichondrium and the tegmen with conchal cartilage.(Fig. 3). An abdominal fat graft was placed in the mastoid cavity. An indwelling myringotomy tube was left in place as a sentinel for continued CSF leakage.
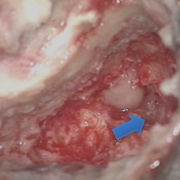
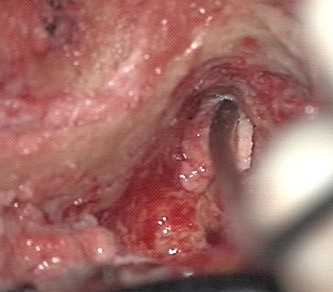
Figure 2 Figure 2
Postoperatively, his drainage immediately resolved and his hearing improved to normal (preoperatively he had a 35 dB conductive loss). He has not re-leaked after 9 months of follow-up and he is very happy.
This case illustrates that CSF leak should be suspected in all cases of chronic refractory otorrhea, even when the drainage is not clear or profuse. The CT was not definitive, and although it did demonstrate a tegmen defect, this is not an unusual finding in chronic ear disease. The surgery proved the diagnosis and allowed a direct route for repair. Temporal bone encephalocele with CSF leak can be treated through a transmastoid approach, with a success rate of about 90%. In an older patient, the transmastoid approach avoids the potential morbidity of a craniotomy. Failures have only occurred in patients with very large defects, chronically elevated ICP, and prior radiation, and these few were successfully treated via transcranial approach.
Case 2. A 55 year old woman complained of pressure and hearing loss in the left ear for >10 years. An otolaryngologist originally diagnosed serous otitis media and performed a myringotomy tube. This led to continuous clear drainage. The tube was removed and the hearing loss recurred. There was no history of headaches, neck stiffness, fever, otalgia, or visual changes. Physical examination revealed clear fluid effusion in the left ear. CT scan revealed diffuse opacification of the mastoid and middle ear, and a small tegmen tympani defect in the anterior part of the epitympanum, near the petrous apex. MRI indicated a small encephalocele at the same location as the tegmen defect, and fluid in the middle ear and mastoid with the same imaging density as CSF. CT-MRI fusion imaging indicated that the leak was coming from this location.
A myringotomy tube was performed and profuse clear drainage resulted. The fluid was positive for beta-2-transferrin. A neurosurgical consult was obtained. A transcranial repair was planned because of the anteromedial location of the leak.
The area was approached through a temporal craniotomy. A lumbar drain was placed and immediately clamped. The tegmen defect and encephalocele were isolated through an extradural approach. The tegmen was repaired with a split calvarial bone graft. An epidural repair or the dura was attempted but the leak could not be controlled because of the medial location of the dural defect. An intradural approach was then performed, with secure placement of a graft of acellular dermis across the dural defect. The repair was reinforced with a layer of abdominal fat and fibrin glue in the epidural space. The dural incision was closed in a watertight fashion, and the craniotomy with titanium mesh. The drain was left open for 3 days and the CSF leak resolved. She was discharged from hospital and did well, with a dry ear and improvement in hearing. The myringotomy tube was left in place as a sentinel.
After 3 months, she complained of intermittent clear drainage from the tube. A fluid sample was positive for beta-2-transferrin. CT-MRI fusion imaging revealed a fluid tract medial to the original repair, at the petrous apex at Meckel’s cave (Fig. 4). A ventriculoperitoneal shunt was performed and the leak resolved.
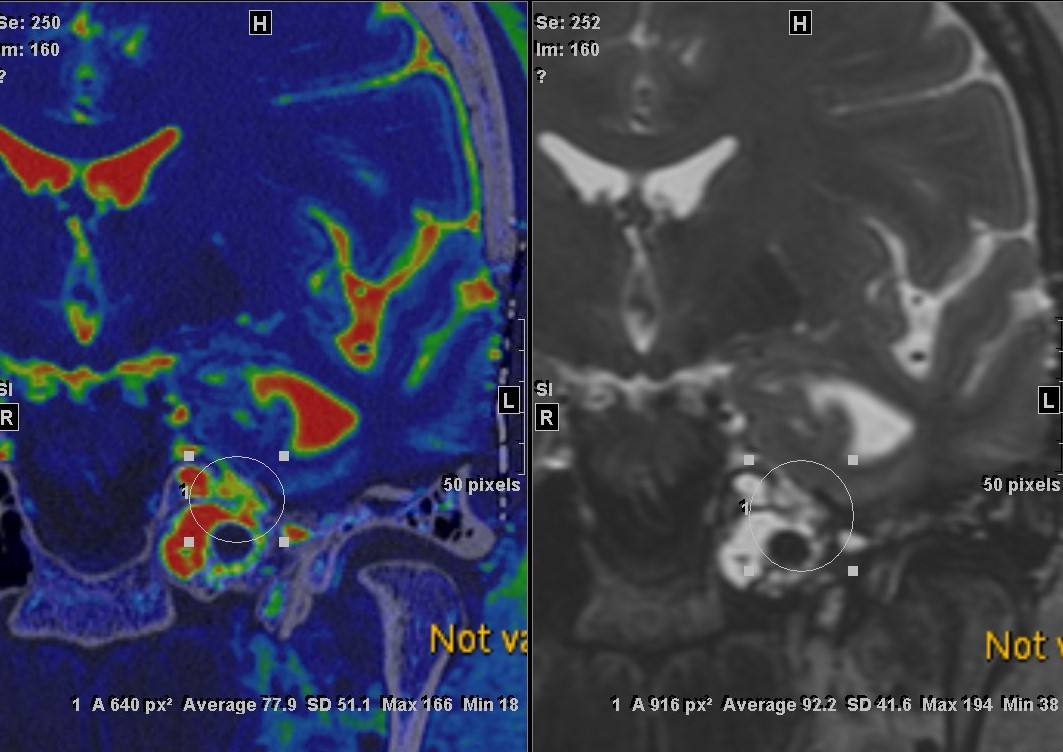
Figure 4
This case illustrates that certain cases of CSF otorrhea can become chronic if they are not diagnosed. A transcranial approach is necessary if the site of leakage cannot be accessed through the mastoid. Increased intracranial pressure may be a cause of failure of direct repain, and may require the placement of a ventriiculoperitoneal shunt.
Complications
- Explain reasons for failure of surgical repair of CSF leak.
- Cite the incidence of meningitis and the role of prophylactic antibiotics.
- Ratilal BO, Costa J, Pappamikail L, Sampaio C. Antibiotic prophylaxis for preventing meningitis in patients with basilar skull fractures. Cochrane Database Syst Rev. 2015 Apr 28;(4):CD004884
Review
- What comorbid conditions are often associated with spontaneous CSF leak?
- What imaging modalities are used to detect CSF leaks in the temporal bone, and what are their virtues and shortcomings?
- What are the advantages of Transmastoid repair of CSF leak over transcranial repair?
- What are the advantages of Transcranial repair over transmastoid?
- What are risk factors for recurrence of CSF leak after surgical repair?
- LeVay AJ, Kveton JF. Relationship between obesity, obstructive sleep apnea, and spontaneous cerebrospinal fluid otorrhea. Laryngoscope 2008;118:275–278
- Pelosi S, Bederson JB, Smouha E. Cerebrospinal fluid leaks of temporal bone origin: selection of surgical approach. Skull Base. 2010 Jul;20(4):253-9
- Carlson ML, Copeland WR, Driscoll CL, Link MJ, Haynes DS, Thompson RC, Weaver KD, Wanna GB. Temporal bone encephalocele and cerebrospinal fluid fistula repair utilizing the middle cranial fossa or combined mastoid-middle approach. J Neurosurg 2013;119:1314-1322
- Eljazzar R, Loewenstern J, Dai JB, Shrivastava RK, Iloreta AM Jr. Detection of CSF Leaks: Is There a Radiologic Standard of Care? A Systematic Review Detection of CSF Leaks: A Systematic Review. World Neurosurg. 2019 Feb 21. pii: S1878-8750(19)30434-6
- Stevens SM, Rizk HG, McIlwain WR, Lambert PR, Meyer TA. Association between lateral skull base thickness and surgical outcomes in spontaneous CSF otorrhea. Otolaryngol Head Neck Surg. 2016:154:707-14
Learner must Sign In to access AAO-HNSF education activities.
- Annual Meeting Webcast (AMW):